

In brief :
- Abdominal diastasis: separation of the abdominal muscles due to stretching of the linea alba, common in pregnancy and postpartum.
- Visible in 50–60% of women at the end of pregnancy or in the weeks following childbirth.
- Mainly functional impact: lower back pain, sensation of instability, limitations in daily movements.
- Realistic prevention: balanced diet, adapted physical activity and posture, without pursuing performance.
- Postnatal rehabilitation is a priority; surgery (abdominoplasty) is reserved for chronic cases and after a stabilized parental plan.
What is abdominal diastasis: mechanisms and clinical illustration
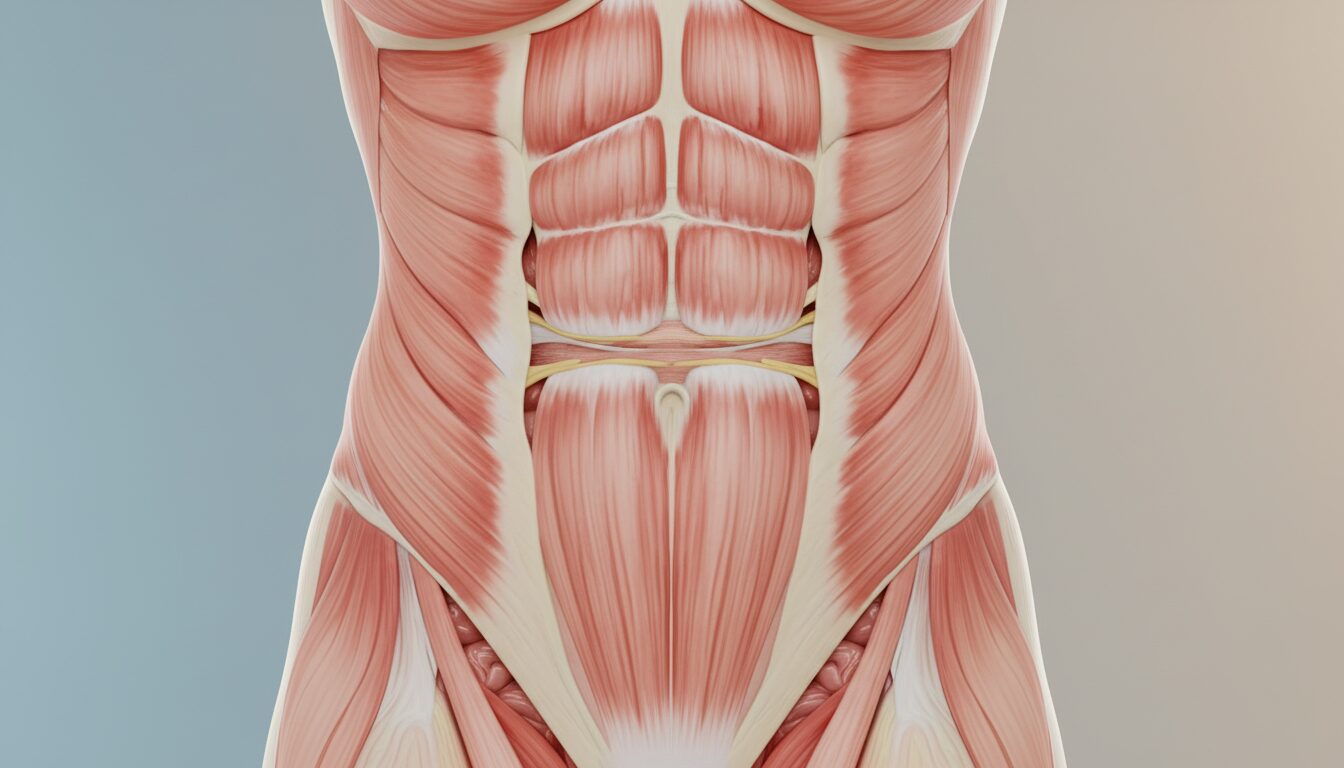
The term abdominal diastasis refers to the separation of the two bundles of the rectus abdominis muscles, linked to the stretching of the central connective tissue, the linea alba. This phenomenon is neither an infectious pathology nor an acute muscle tear: it is a distension. During pregnancy, the increase in the size of the uterus exerts constant forward pressure, forcing the fibers to move apart to make room for the baby. It is a physiological process, sometimes amplified by other factors.
To make the description concrete, here is the guiding thread: Sophie, 33 years old, is expecting her second child. At the end of pregnancy, her belly forms a dome more pointed than round. After childbirth, when attempting a slight sit-up, she perceives a space between the two muscle edges at the navel. This example illustrates the typical presentation of a rectus diastasis.
Understanding anatomy to act better
The linea alba is connective tissue that connects the two rectus abdominis muscles. Its elasticity normally allows it to withstand abdominal pressures. When this line stretches beyond a certain threshold, muscle separation appears. In newborns, especially premature babies, this line is not yet consolidated. In adults, it is often an event linked to pregnancy or rapid weight gain.
Terminology and clinical nuances
Diastasis is not necessarily synonymous with irreversible aesthetic sagging. There are degrees: from slight widening that often resolves within a few weeks, to more pronounced separation that persists and produces a notable functional impact. It is important to distinguish diastasis from a parietal hernia: a hernia involves a rupture with organ protrusion, whereas diastasis is a distension without a clear opening.
Understanding these mechanisms helps avoid panic and propose appropriate actions: observation, protection, and graduated interventions depending on symptom intensity. Key: consider diastasis as a signal of decreased abdominal belt capacity, not as a bodily fault.
Insight : seeing diastasis as a bodily adaptation with options to regain comfort is an essential first step.
Signs, diagnosis, and risk factors of rectus diastasis
Detecting an abdominal diastasis does not always require sophisticated medical equipment. After childbirth, a simple self-assessment can alert: lying on your back, slightly raising your head, placing a hand above and below the navel can feel a soft space or a “gap” between the edges of the abdominal muscles. If this gap is palpable over two to three fingers or more, it is useful to discuss it with a midwife or a physiotherapist specialized in postnatal rehabilitation.
Some functional signs often accompany the aesthetic complaint: lower back pain, quick fatigue during household chores, feeling of crushing or bloating, difficulty carrying the baby for several minutes without discomfort. These manifestations relate to the functional impact of diastasis.
Factors promoting onset
Several elements increase separation risk: multiparity, maternal age over 34 years, significant weight gain during pregnancy, multiple pregnancy, cesarean delivery, or lack of adapted activity. Fetal size (macrosomia) and large abdominal circumference at the end of pregnancy also contribute. These factors act by increasing internal pressure and overloading the linea alba.
When to consult?
Consultation is recommended if symptoms disrupt daily life (chronic pain, limitations in parental movements), if a suspicious mass appears locally, or if separation persists for several months despite conservative measures. The professional will often use palpation, clinical evaluation, and if needed, ultrasound to measure the gap.
Concrete example: Sophie waited six weeks postpartum before consulting. The midwife confirmed a moderate gap and referred her to specialized physiotherapy. This pathway illustrates the most common approach: evaluation, rehabilitative care, and regular reassessment.
Insight : spotting signs early and seeking advice helps avoid chronicity and preserves maternal health.
Functional impact: pain, posture, and daily life after childbirth
Abdominal diastasis has repercussions that go beyond the appearance of the belly. The separation of the rectus muscles weakens the abdominal belt, reducing the ability to stabilize the pelvis and lumbar spine. The result often shows as lower back pain, decreased muscular endurance, and discomfort in daily activities: carrying the baby, bending to pick up an object, lifting a child. These limitations affect quality of life and body confidence of new mothers.
Consider Sophie’s case again: she avoided picking up the baby’s toys for fear of worsening her belly. This restriction fueled anxiety and additional fatigue, illustrating how diastasis can impact mental health and family routines.
Mechanical and postural consequences
Loss of anterior support forces the rest of the body to compensate. The back may carry more load, shoulders slump, and diaphragmatic breathing may be impaired. These adaptations favor chronic pain if nothing is done. Moreover, repeated bad movements (pushing with the belly or holding the breath during exertion) can maintain or even worsen the separation.
Practical strategies to limit immediate impact
Some simple gestures, validated in clinical practice, improve daily management: learning to straighten up by rolling on the side rather than rising while tightening the belly, carrying the baby close to the body, favoring breastfeeding positions that don’t pull on the linea alba, and taking frequent breaks. These adaptations reduce pain and preserve functional capacity while awaiting postnatal rehabilitation.
On the emotional level, a guilt-free approach is essential: reminding that the body has just undergone a major change and it is normal to need time and support. Contact with other parents who have gone through the same often proves reassuring and motivating.
Insight : diastasis has a real impact on daily life, but simple gestures and targeted support quickly limit functional consequences.
Prevention during pregnancy and postnatal rehabilitation: concrete actions and treatments
Prevention of abdominal diastasis during pregnancy relies on realistic and caring measures. There is no absolute guarantee, but several habits reduce the risk of excessive widening: maintaining adapted physical activity, hydration, balanced diet, and attention to posture. These measures promote tissue tone and limit excessive weight gain, an aggravating factor.
Practical advice for pregnancy
- Practice regular adapted activity (walking, prenatal yoga, aqua aerobics) to preserve tone without straining the abdominals.
- Train your supports: learn to get up from the floor without sudden effort, use gluteal muscles to push rather than the belly.
- Avoid classic abdominal exercises late in pregnancy (sit-ups, crunches) that promote widening.
- Stay hydrated and eat a varied diet to support connective tissue quality.
These tips can be presented as a short personalized plan, developed with a midwife or a professional in perinatal education.
Postnatal rehabilitation and therapeutic options
After childbirth, postnatal rehabilitation is the most common and least invasive intervention. It aims at progressive muscle strengthening, diaphragmatic coordination, and posture rehabilitation. Specialized physiotherapists offer targeted exercises: safe activation of the transverse abdominis, breathing work, pelvic bridges, and functional integration. These sessions often significantly reduce the gap and improve comfort.
Surgery (abdominoplasty) is an option for persistent and bothersome diastases, when the pregnancy plan is complete. It surgically brings the muscles together under anesthesia and requires convalescence, sometimes with limited coverage by healthcare systems according to criteria. Wearing a girdle is often recommended after surgery.
Comparative table of approaches
| Approach | Objective | Advantages | Limitations |
|---|---|---|---|
| Postnatal rehabilitation | Functional strengthening and coordination | Safe, progressive, improves pain and function | Requires time and regular commitment |
| Support girdle | Temporarily stabilize the abdominal wall | Immediate effect on comfort | Does not replace rehabilitation |
| Abdominoplasty | Definitive anatomical correction | Marked aesthetic and functional result | Surgery, convalescence, not for future pregnancy plans |
For Sophie, the chosen path was progressive physiotherapy care, combined with postural advice and easy daily exercises integrated into the child-baby routine. Six months later, her comfort and body confidence had markedly improved.
Practical list to try today :
- Diaphragmatic breathing 3 times 1 minute upon waking.
- Get up from the floor by rolling onto the side to protect the linea alba.
- Carry the infant close to the body and alternate arms.
- Consult a specialized physio if pain or gap noticeable over 2 fingers or more.
Insight : adapted rehabilitation and simple daily gestures often provide significant improvement without invasive intervention.
What are the differences between diastasis and hernia?
Diastasis is a separation of the linea alba without a breach allowing organ passage; hernia involves an actual opening of the wall and may require urgent surgery. Clinical diagnosis and ultrasound allow distinction.
When to start postnatal rehabilitation?
Rehabilitation can start in the first weeks after delivery according to healthcare professional advice. An initial assessment by a midwife or physiotherapist is recommended to adapt the program.
Can abdominal diastasis be totally prevented during pregnancy?
There is no absolute prevention, but maintaining adapted activity, a balanced diet and good posture reduces the risk and severity of muscle separation.
Is surgery covered?
Aesthetic surgery (abdominoplasty) is generally conditional on the absence of future pregnancy plans, and its coverage by Social Security depends on specific medical criteria. Medical advice is essential.


